There can be various problems that can occur within the spinal column, cord or the nerves that could affect the smooth function of this amazing structure. The problems could range from minor “wear and tear” known as degenerative conditions to more sinister conditions such as tumours. The other condition that could affect the spine includes infection, disc prolapses, traumatic fractures, osteoporotic fractures, vascular malformation and developmental problems such as spinal lipoma and tethered cord syndrome.
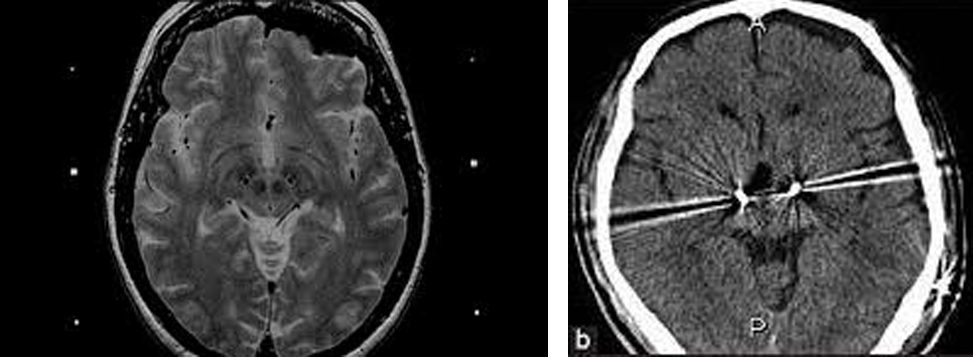
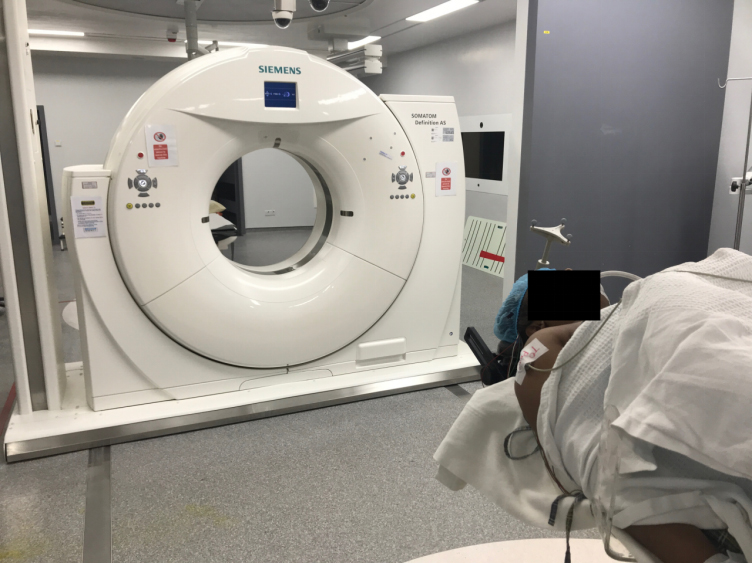
These problems need to be evaluated clinically by taking a good history and complete physical examination. Then the relevant investigations need to be conducted eg. X rays, CT scan, MRI scans, nerve conduction studies etc. The MRI images are of high resolution (1.5 to 3.0 Tesla). Once the exact problem has been identified, the management strategy is formulated that is suitable to that particular patient considering all factors eg. age, medical background, degree of disability etc.
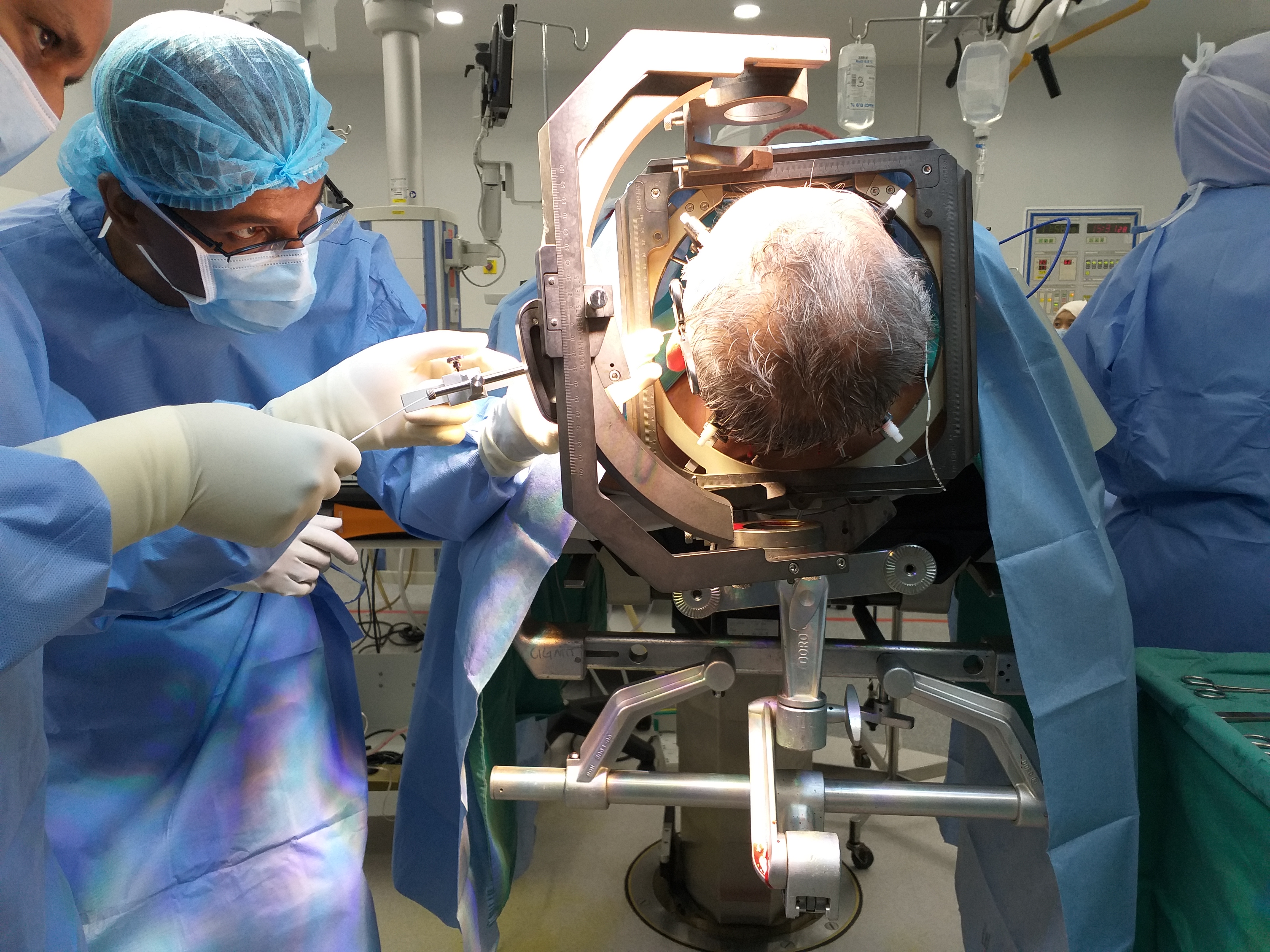
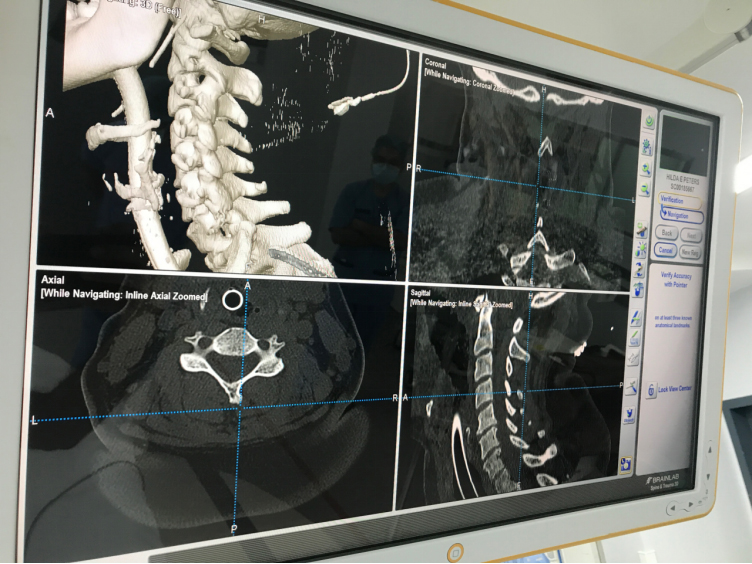
The surgical treatment is varied depending on the condition. It is carried out in operation theatre mostly under general anaesthesia. The “state of the art” equipments are available at our disposal and are used for the cases in order to obtain the best possible outcome. The equipment available to be used includes high end microscope, BRAINLAB image guidance system, intraoperative neurophysiological nerve monitoring, endoscopes, ultrasonic aspirators etc.
Post operative recuperation is managed with adequate analgesia eg oral analgesic, patient controlled analgesic (PCA) etc. Few days after surgery, physiotherapy and rehabilitation therapy is instituted.
There are host of paediatric neurosurgical problems that can affect a newborn, infant, toddler, teenager and adolescence. When the baby is born with a particular condition is known as a congenital condition. However, if the baby is born normal but over the years develop a condition it is an acquired or developmental condition.
Paediatric neurosurgical services would admit children between the ages of a newborn up to the age of 18 years old. The conditions that affect children vary with the age group which may involve the brain or the spinal cord.
The newborn may have congenital conditions example protrusion of a sac or brain from the defected skull or spine, abnormal lumps, dimples or hairy patches at the lower back, enlarging head circumference, abnormal skull shape etc. These various conditions of meningoencephalocele, spinal lipoma, hydrocephalus, tumours and craniofacial syndromes need urgent neurosurgical attention.
The older child may develop progressive unsteadiness on the feet, seizure, weakness, blurring of vision, persistent vomiting etc. These are symptoms of a possible brain or spinal cord problem eg. brain tumours, spine tumours, abnormalities in the spine formation etc. These problems need to be evaluated clinically by taking a good history and complete physical examination. Then the relevant investigations need to be conducted eg. X-rays, Ultrasound scans, MRI scans, nerve conduction studies etc. The MRI images are of high resolution (1.5 to 3.0 Tesla). Once the exact problem has been identified, the management strategy is formulated that is suitable to that particular patient considering all factors eg. age, bone maturity, and weight of the child etc.
The common conditions treated in the unit range from congenital problems of brain and spine eg. meningoencephalocele, spinal lipoma etc; developmental problems etc. craniocervical problems; brain tumours; spinal tumours; hydrocephalus; craniosynostosis (non-syndromic and syndromic) and traumatic brain and spinal injury.
There is a multidisciplinary team to deal with craniofacial cases which compose of neurosurgeons, maxillofacial surgeons, ENT surgeons, eye surgeons, geneticist, paediatric intensivist, paediatric anaesthetist, physiotherapist, social worker etc.
The surgical treatment is varied depending on the condition. It is carried out in operation theatre mostly under general anaesthesia. The “state of the art” equipments are available at our disposal and are used for the cases in order to obtain the best possible outcome. The equipment available to be used includes high-end ZEISS microscope, electromagnetic MEDTRONIC AXIEM S7 image guidance system, neurophysiological intraoperative nerve monitoring, endoscopes, ultrasonic aspirators etc.
The post-operative care is carried out in the intensive care unit or high dependency unit depending on the condition. The brain and spinal tumour cases are jointly managed with the paediatric oncologist.
The patients are followed up in the clinic periodically to assess their clinical condition and well being. Some patients would also require serial imaging eg MRI scans.
The Functional Neurosurgery Service of UMMC & UMSC offers surgical treatments such as Deep Brain Stimulation (DBS) for movement disorders and other related conditions.
The service also offers a full range of stereotactic procedures including lesioning.
Examples of conditions treated include Parkinson’s disease, tremulous disorders and dystonic conditions as well as other more unusual movement disorders. The group runs inter-specialty joint clinic consultations involving neurosurgery and neurology for patients with complex movement disorders referred for DBS surgery.

Utilising the Novalis Tx Radiosurgery systems with state-of-the-art technology that integrates treatment planning in one system. A one of a kind technology that can treat both non-cancerous and cancerous conditions in a very less time is known as Novalis Tx radiosurgery system. Novalis radiosurgery accurately shapes the radiation beam to the area to be treated and uses imaging guidance and other methods to target the tissue or tumor to be treated while avoiding surrounding healthy tissues. Stereotactic radiosurgery is a non-invasive process that delivers high doses of radiation on the tumor from different angles.
Novalis Tx is an ideal technology for treating those tumors that were previously located in inaccessible locations and were difficult to treat. This technology decreases the treatment time as the high-dose radiation beams matches the shape of the tumor that is being treated. The potential errors are also reduced as in the case of time consuming procedures. The entire treatment session can be completed in just 15 minutes.
Applications:
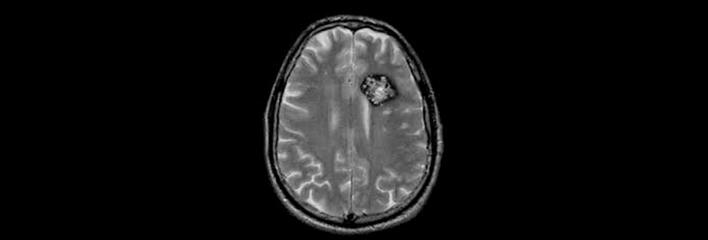
- Neuro-oncology – Brain (Extra-axial and Metastatic Tumours) and Spine (Intradural- Extramedullary & Intramedullary).
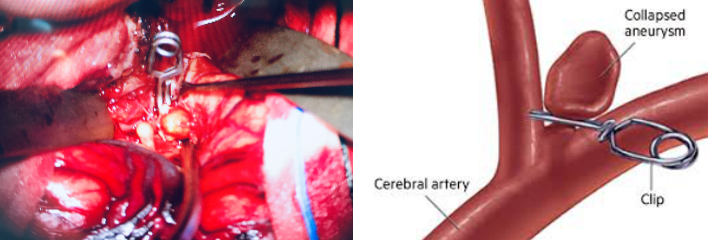
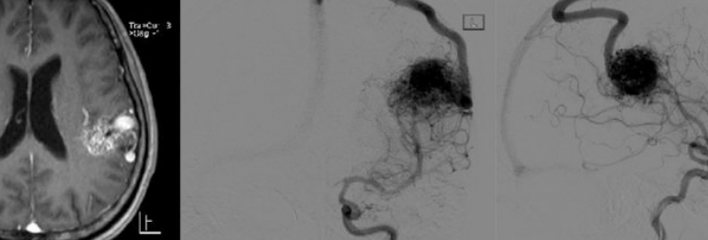
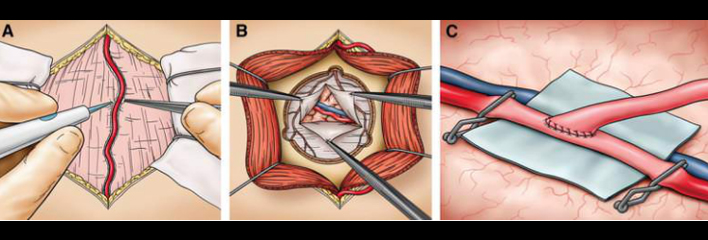
- Vascular Neurosurgery – management of inoperable or eloquently located arterio-venous malformations and angiographically occult vascular malformations.
- Craniofacial Pain Syndromes – In the Management of Trigeminal Neuralgia, and other Cephalic Neuralgias.
- Skull Base Neurosurgery – As a Primary and Secondary Treatment Modality in management of cerebellopontine angle tumours, petrosal tumours, sellar lesions and paragangliomas.
- Pituitary Tumours & Craniopharyngiomas.
- Other Applications – Novalis Tx radiation therapy has also applications in thetreatment Seizures, Parkinson’s disease, Obsessive Compulsive Disorder and Cluster Headaches.
Application in Neuro-oncology
While surgery generally but not invariably remains the primary and definitive management in neuro-oncology, in both Primary and Stereotactic Radiation Therapy, both Stereotactic Radiosurgery (SRS) and Stereotactic Radiotherapy (SRT) are increasingly becoming an adjunct tool in the management of the same and increasingly replacing surgery as the primary modality of treatment.
The utility and indications of SRS and SRT in our Centres is Evidence Based
Since the launch of Radiosurgery Services at UMMC in 2015, Stereotactic Radiation Therapy is only selectively not given to excised tumour beds in cerebral metastasis, where in radiation therapy is not the primary management.
Stereotactic Radiosurgery is also used as adjuvant therapy in the management of Benign Tumours of higher grades viz Atypical Meningiomas.
Application in Vascular Neurosurgery
The Spetzler-Martin Classification is an arbitrary system that stratifies the complexity of arteriovenous malformations (AVMs) with regards to surgery based on their size, eloquence of location and the veins the malformations drain into.
Before the advent of stereotactic radiation therapy, high grade AVMs where either managed expectantly, or were associated with significant surgical morbidity. With the evolution of Stereotactic Radiation Therapy, high grade complex AVMs have been treated successfully through single treatments, the application of fractionations or the staging of treatment utilizing both applications.
The management of brainstem and thalamic angiographically occult vascular malformations namely Cavernomas with stereotactic radiation therapy to decrease the incidence and frequency of haemorrhages, has become evidence-based.
Application in Craniofacial Pain Syndromes.
Craniofacial Pain Syndrome is increasingly becoming prevalent in our population. When there is an absolute or relative contraindication for Surgical Microvascular Decompression, Stereotactic Radiosurgery is increasingly being utilized ahead of more invasive techniques such as percutaneous trigeminal rhizotomy – radiofrequency ablation and glycerol injections
Application in skull base surgery
In UMMC & UMSC, virtually all Vestibular Schwannomas (Acoustic Neuromas) less then 3cm in size with hearing impairment and no brainstem compression have been treated successfully with stereotactic radiosurgery. A definite treatment algorithm exists for treatment of larger lesions with Microsurgery or Hyperfractionated Stereotactic Radiosurgery.
A series of Paragangliomas mainly Glomus Tympanicum and Glomus Jugularae have been treated successfully as the primary modality of treatment at our Centres since 2015.
Stereotactic radiation therapy is also rapidly becoming a treatment modality for pituitary tumours and Craniopharyngiomas. In our Centres, Radiosurgery is employed when Surgical and Medical Therapies fail to achieve Biochemical Cures in conditions of Functioning Pituitary Adenomas namely, Acromegaly, Cushings’ Disease and Prolactinomas.
Craniopharyngiomas though histologically benign, are tumours composing of solid and cystic component that arise from the pituitary stalk. They are difficult to cure, making them malignant in behavior. A series of residual and recurrent Craniopharyngiomas following surgery treated with Radiosurgery at our Centres have shown good control of the cystic and solid components of these residual /recurrent tumours.
 |
 |
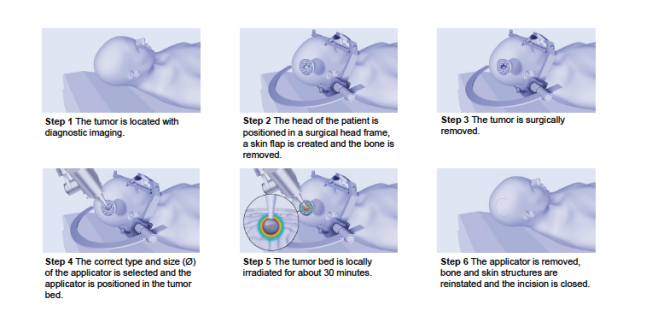
- Intraoperative radiation therapy (IORT) is an intensive radiation treatment that’s administered during surgery. IORT allows direct radiation to the target area while sparing normal surrounding tissue. In UMMC & UMSC IORT is used to Brain Metastases where there is a concern that microscopic amounts of cancer may remain.
- A miniature and mobile X-ray source which emits low energy X-ray radiation in isotropic distribution. Due to the higher ionization density caused by soft X-ray radiation in the tissue, the relative biological effectiveness of this low-energy X-rays on tumour cells is higher when compared to high-energy X-rays or gamma rays.
-
In the future we are aiming to be able to provide this emerging technique to treat primary and metastatic brain tumors that can be hard to reach with conventional surgery.
LITT is performed by implanting a laser catheter into the tumor and heating it to temperatures high enough to kill the tumor, while HIFU is a non-invasive therapeutic technique that uses non-ionizing ultrasonic waves to heat tissue and ablate the lesion.